Conclusions on the status quo in the logic of medical language regarding the masticatory system
Conclusions on the status quo in the logic of medical language regarding the masticatory system
Abstract: The "Introduction" chapter explores the evolution of diagnostic practices in the masticatory system, focusing on the epistemological challenges of shifting paradigms. Drawing from scientific philosophies, particularly Kuhn's theory of paradigm shifts, the chapter addresses the inherent resistance to new ideas, often caused by the disruption of established power structures. The primary concern, however, is the impact on patients, as outdated diagnostic methods can hinder accurate diagnosis and treatment.
This chapter outlines the critical need for standardized nomenclature and interdisciplinary approaches to overcome diagnostic errors. It highlights the complexity of the diagnostic process, where multiple stakeholders, including the patient, clinicians, and healthcare systems, must collaborate effectively. The chapter also discusses the role of epistemology and interdisciplinarity in fostering clearer diagnostic models, emphasizing the importance of a scientific method that incorporates formal methodologies rather than subjective descriptions.
A key point in the discussion is the limitations of classical probability models, particularly the P-value, in accurately reflecting the complexities of biological systems. The chapter introduces the idea of quantum-like diagnostics, which, while not rooted in quantum particle physics, borrow probabilistic approaches to more accurately model biological processes. This is exemplified by a practical case study involving the evaluation of occlusal conditions and neurophysiological responses.
Finally, the chapter sets the stage for introducing a new diagnostic model called "Index Ψ," which aims to integrate neurophysiological data to evaluate the trigeminal system and determine whether a patient is in "Normocclusion" or "Malocclusion." The chapter closes by emphasizing the importance of continuing treatment with a clear neurophysiological understanding, marking a shift towards a more informed and precise approach to dental and masticatory diagnostics.
Introduction
After a lexical path concerning the status quo in the field of diagnostics of the masticatory system, sometimes apparently off topic, we have reached the stage in which all the discourses crystallize in clinical practice and therefore we will try to explain the reason for so much dialectical length.
First of all, we can defend this strategy of conceptual exposure with the difficulty of the change of mindset which is generally innate in the human being, like Kuhn explains so clearly in his scientific philosophy of 'Paradigms'. He taught us that the new paradigms, namely the 'Extraordinary Science', generate tenacious opponents to their acceptance. This is also justifiable, because there are a myriad of storytellers around, although it is also true that the new paradigms destabilize the acquired power and that is why they are often rejected even by confirmed cultural environments.
Having said that, however, the fact is that here there is a human being called 'Patient' involved, and the restriction of the cultural and progressive field does not go to the detriment of the man of power (a professor, a politician, ...) but exclusively of the patient. Since the project follows the Feyerabend philosophy, as already said in previous pages, Masticationpedia shows all its loyal, democratic and ethical scientific thinking with ideas, facts and clinical cases, the rest will be time to judge the veracity of the project.
Diagnostic errors and causes
Medical errors diagnose as much as the axioms on which therapeutic models are based are continually clashing between titans of the clinical scientific scene as some studies on the subject point out:
- The lack of standardized nomenclature and overlapping definitions of medical errors has hindered the analysis, the synthesis and data evaluation.[1]
- The diagnostic process is collaborative and involves the patient, the clinician, the healthcare system and its various stakeholders [2]
- Contributing factors associated with misdiagnosis included dentist knowledge and skills, inadequate time, lack of communication between colleagues, and cognitive biases such as premature closure based on prior experience. Some participants perceived that an error only occurs when the choice of treatment leads to harm. The strategies suggested by the participants to prevent these errors required adequate time to investigate a case, form study groups, increase communication, and place greater emphasis on differential diagnosis.[3]
These three bibliographic references were enough to extrapolate some essential concepts such as:
- standardized nomenclature, which presupposes the need for formal methodologies, like in mathematical and physical sciences, and not subjective and/or exclusively descriptive models.
- the diagnostic process understood as an 'Observable' in which several elements are involved, such as the observer, the measuring instrument, the patient as well as the ability to interpret verbal language and decode the encrypted signal of the observed system;
- place greater emphasis on differential diagnosis, a key element that we will try to demonstrate practically with some cases mentioned in the previous chapters.
A coherent language
These quotations and questions have led us to a more appropriate and profound description of the topics covered in the previous chapters, because we cannot talk about standardized nomenclature, diagnostic process and differential diagnosis without talking about:
- Epistemology of knowledge
Epistemology (from the Greek ἐπιστήμη, epistème, "certain knowledge" or "science", and λόγος, logos, "discourse") is that branch of philosophy that deals with the conditions under which scientific knowledge can be obtained and the methods to achieve such knowledge. The term specifically indicates that part of gnoseology that studies the foundations, validity and limits of scientific knowledge.
In fact, an almost unlimited value has been given to a statistical test such as [4][5][6] and to the statistical data of a 'Classical Probability' based on Bayes' Theorem (which we will discuss in the next chapters)[7] and then witness a relative brake on the subject [8][9] and all that is 'Epistomology', that almost spontaneously highlighted another fundamental passage that of 'Interdisciplinarity', a phenomenon that only with great effort is recognized as important as the specialized disciplines.

- Interdisciplinarity
The proposed alternative philosophical paradigm, called the "Engineering Paradigm of Science" implies alternative philosophical assumptions regarding aspects such as the purpose of science, the character of knowledge, the epistemic and pragmatic criteria for the acceptance of knowledge and the role of technological tools. Consequently, scientific researchers need so-called metacognitive scaffolds to aid in the analysis and reconstruction of how "knowledge" is constructed in different disciplines. [10][11] Precisely these 'Metacognitive Scaffolds' have allowed us to consider an important requirement in diagnostics that of 'basic knowledge' which tends to reduce the vagueness and ambiguity of the logic of medical language.[12]
- Logic of medical language
These premises [13] [14] led us to the description of 'Fuzzy logic' models in which the 'Basic knowledge' is stratified at multiple levels of the context in multiple disciplines, increasing its capacity in differential diagnosis. All this is Logic of medical language' with which we followed the diagnostic process of our poor patient 'Mary Poppins' who for 10 years hoped to be made a certain diagnosis despite the various attempts of clinical scientific propositions in the dental and neurological context:
Propositions in the Dental Context
Positive radiological report of the TMJ in Figure 2

Positive CT report of the TMJ in Figure 3

Positive axiographic report of the condylar traces in Figure 4

Asymmetric EMG interference pattern in Figure 5

Propositions in the Neurological Context
Jaw jerk in Figure 6

Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle {\displaystyle \gamma _{2}}=} Mechanical Silent Period in Figure 7
Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle {\displaystyle \gamma _{3}}=} CT right masseter muscle in Figure 8
Propositions in the Dental Context

Figure 1: Patient in entry in the Functional Neuro Gnathology Department who reported right hemilateral orofacial pain for 10 years with previous diagnosis of Temporomandibular Dysfunction.


Figure 2: Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle \delta_1=} Patient's TMJ Stratigraphy showing signs of condylar flattening and osteophyte

Figure 3: Computed Tomography of the TMJ showing the flattening of the TMJ
Figure 4: Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle \delta_1=} Axiography of the patient showing a flattening of the chewing pattern on the right condyle

Figure 5: Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle \delta_2=} EMG Interferential Pattern. Overlapping upper traces corresponding to the right masseter, lower to the left masseter.




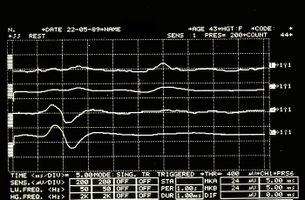
Figure 6: Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle {\gamma _{1}}=} Jaw jerk electrophysiologically detected on the right (upper traces) and left (lower traces) masseters
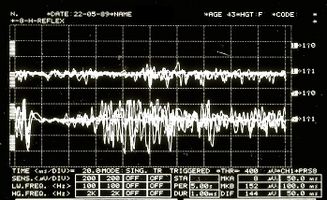
Figure 7: Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle \gamma _2=} Mechanical silent period detected electrophysiologically on the right (upper overlapping traces) and left (lower overlapping traces) masseters
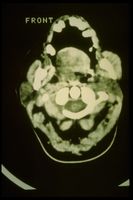
Figure 8: Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle \gamma _3=} CT shows evident hypertrophy of the right masseter
Figura 9: Patient in leaving from the Functional Neuro Gnathology Department after 1 week with differential diagnosis of 'Hemimasticatory Spasm'



Any colleague, even if of excellent clinical preparation in his own exclusive scientific dental context, would have had considerable difficulty in making a differential diagnosis between 'Temporomandibular Disorders' and 'Neuromotor Damage' without implementing his 'basic knowledge' on the exclusively neurophysiological phenomenon of Synaptic trasmissione in the dedicated chapter. Here, in fact, the limits of the Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle P-value} , classical probability and Bayes statistical processes referring to specific contents of the discipline in question.
- The encrypted code sent out by the trigeminal system, the one to be decrypted, was:
(we will discuss it extensively in the chapter 'Hemimasticatory Spasm')
Already serious complexities of medical reality and difficulties of an ambiguous and vague logic of language, are worsened by additional problems related to the peculiar interpretation of the phenomena, an approach which is substantially dichotomous: a phenomenon that is physical, chemical or biological, can be interpreted through a deterministic mindset (a 'cause/effect only', one) which falls into a classical probability, or prefers an exclusively probabilistic description of the reality, called quantum probability.
After these considerations, we have proposed to think of a superposition of states in a system, starting a priori from the solid belief that an asymptomatic subject is simultaneously healthy and sick, until the 'Observable' is measured through an instrument. Leaving aside the various possible interpretations, the collapse of orthodox thought will be caused by its interaction with a macroscopic measuring object; that is when this 'Observable' is observed by the observer.
We have therefore generated an 'Observable' (which includes the physical state of the system itself), an observer and a measuring instrument.
Introduction to quantum-like diagnostics
As already described in the dedicated chapters, the quantum-like strategy exclusively concerns the epistemological and probabilistic aspect, and has no correlation with the typical characteristics of quantum particle physics, although it extrapolates probabilistic mathematics. To be precise, the formula Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle \psi(t_1)=|1\rangle |vivo \rangle + |0\rangle |morto \rangle} is not complete: we have to multiply each term to the right of the equation with a number. The number indicates the 'probability' that the specific event will occur, the complete formula will then be:
Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle \psi(t_1)=\sqrt{p_1}|1\rangle |alive \rangle + \sqrt{p_0}|0\rangle |dead \rangle}
The number indicates the (square rooted) probability that the specific event will occur.
Let's take an example that brings us back closer to the medical field:
If the event Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle |1\rangle |healty \rangle} has a 50% chance of occurrence and the event Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle |0\rangle |sick \rangle} has 50% to occur then the formula becomes (less than phase factors)
Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle \psi(t)=\sqrt 50%|1\rangle |healthy \rangle + \sqrt 50%|0\rangle |sick \rangle}
which in more exact mathematical terms turns into
Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle \psi(t)=\sqrt 0.5|1\rangle |healthy \rangle + \sqrt 0.5|0\rangle |sick \rangle}
In this way, two other limits of laboratory diagnostics measuments are deduced: that of Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle K_{brain}} analogous values to the Heisenberg uncertainty principle, suggesting a common underlying architecture of human brain activity in resting and task conditions and classical probability vs quantum probability which substantially cast indecision on the interpretation of clinical and diagnostic phenomena.
A practical example
Let's spend a minute to take a look at this example:
| Entry level: | Malocclusion | Normocclusion |

Figure 10a: Patient in entry in the Functional Neuro Gnathology department referred by colleagues for orthodontic and orthodontic treatment.
Orthodontically speaking, it would be irreverent not to consider the patient in a state of malocclusion. According to orthodontic canons, this is a case that has to be treated both orthodontically and surgically to restore a hypothetical 'Normocclusion';
yet, we will see that the reality is quite different
Figure 10b: Patient in entry in the Functional Neuro Gnathology department, referred by colleagues for a prosthetic rehabilitation of edentulous mandibles considered to be in a condition of 'normal occlusion' after having been surgically treated with a bimaxillary orthognathic intervention.
The patient, therefore, would find himself in a condition of 'Normocclusion;
yet, we will see in this case too that the reality is quite different.


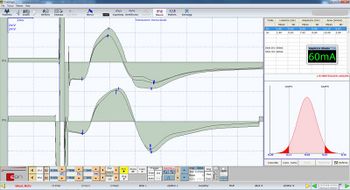
Figure 11a: Determination of the (structural or organic) anatomical symmetry of the patient's motor trigeminal nervous system in figure 1 with Malocclusion. The area of the graph (latency-amplitude) gives for the right side the value 13.15 mV / ms, for the left side a value of 13.60 mV / ms
This indicates a symmetry difference of 0.8%.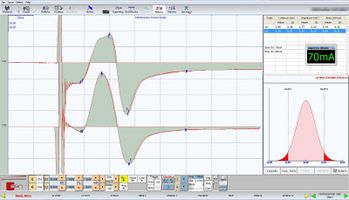
Figure 11b: Determination of the anatomical symmetry of the patient's nervous system "figure 1 malocclusion". The graph area (latency-amplitude) gives for the right side the value 9.7 mV / ms for the left side a value of 9.69 mV / ms.
This indicates a symmetry of 0.1%.
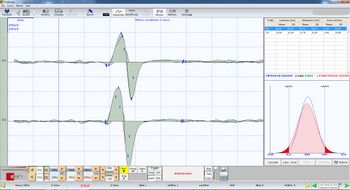
Figure 12a: Determination of the functional component of the Central Nervous System. The results for patient 1 malocclusion show an area of 1.34 mV / ms and 1.46 mV / ms on the right and left masseter respectively.
This shows a symmetry difference of 8.2%.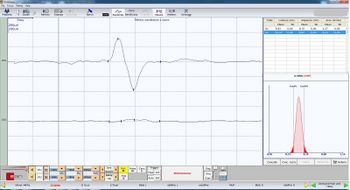
Figure 12b: Determination of the functional component of the Central Nervous System. Results for patient 2 (normocclusion) show an area of 1.37 mV / ms and 0.13 mV / ms on the right and left masseter, respectively.
This shows a 90.5% symmetry difference.


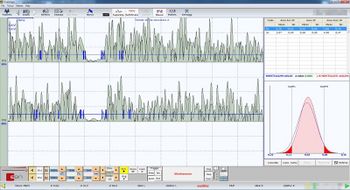
Figure 13a: Execution of the Mechanical Silent Period showing perfect symmetry both in latency and duration as well as a well represented post-inhibition integral area.
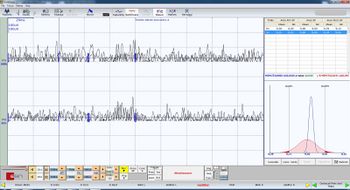
Figure 13b: Lack of the masseterine mechanical Silent Period on both sides which demonstrates the evident lack of motor neuron recruitment from occlusal instability.


Figure 14a: Patient in 'exit' from the Functional Neuro Gnathology department with referencing of 'Occlusal dismorphism' and not of 'Malocclusion'
Figure 14b: Patient in 'exit' from the Functional Neuro Gnathology department with severe 'Malocclusion' report to be treated immediately.
| Exit level: | Normocclusion | Malocclusion |
In the end, after having somehow considered the axiomatic certainties and deterministic significances in a diagnostic context as critical (Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle P-value} ), and having proposed a quantum probability model that in broad lines follows the path of the Bayes Theorem by adding an interference element (see Khrennikov) in the dedicated chapter, obviously an Hamletic doubt arises
Towards a model
The model presented here above, of course, is remarkably complex because in this context only the conceptual procedure to follow has been presented: we will see later in the course of reading that everything will materialize in an interesting modeling of the trigeminal electrophysiological responses from which a clinical mesoscopic model will be created, of which we can already anticipate the name: 'IndexFailed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle \psi} .
Through this Index Failed to parse (MathML with SVG or PNG fallback (recommended for modern browsers and accessibility tools): Invalid response ("Math extension cannot connect to Restbase.") from server "https://wikimedia.org/api/rest_v1/":): {\displaystyle \psi} we wikk be able to evaluate in detail, and quickly, the state of the trigeminal system, as well as to consider whether the patient is in 'Normocclusion' or in 'Malocclusion'
Having said this, however, there is a clarification to avoid falling into misunderstandings such as:
Well, this is not at all the moral of the story, we would say, instead:
«Yes, of course, we will continue to treat patients, but now we will do it knowing what we are doing from a neurophysiological point of view.»
Another example
Just for the sake of completeness.
Figure 15a shows the previously presented patient undergoing orthognathic surgery; at a first electrophysiological check he showed a wide asymmetry of the reflexes, with lack of the masseterine silent period. This led us, therefore, to confirm the occlusal state of 'Malocclusion'. This could give rise to the above said misunderstandings because, actually, orthognathic will never be able to respect the neurophysiological conditions in an appropriate way: the interventions are complex and must be performed in a condition of curarization that cancels the neuromotor component.
The orthognathic, therefore, intrinsically has a critical limit: the cancellation of the neuromotor component, and still it must necessarily follow the anatomical and occlusal canons. The fact is that, frequently, the anatomical and neuromotor conditions coincide, returning a perfectly successful model from an aesthetic, functional and neuromuscular point of view; but sometimes the pre- and operative conditions prove unsuccessful in this aim.
The occlusal position, and therefore the 'Centric Relationship'[15], necessarily depend on the spatial position of the TMJ and of the mandible after surgical reduction. The finalization procedures, therefore, through anatomical maneuvers, such as the centric recordings, will necessarily return the spatial position appreciated in figure 15b.

Figure 15a: Patient in exit from the Functional Neuro Gnathology department with severe 'Malocclusion' report to be treated immediately.

Figure 15b: Higher magnification detail to visualize the mandibular incisal position after orthoneurognathic intervention

Figure 15c: Detail at higher magnification to visualize shifting of the mandibular incisal position through 'Neuro-evoked Centric Registration'


As previously mentioned, for each problem the code to decrypt should be found, and in this case it is the curarization, that has canceled the neuromotor component; consequently, it is from here that we must start to recover the component.
By performing a neuro evoked Centric recording through a technique of 'Transcranial Electrical Stimulation' of the trigeminal motor roots, the mandibular spatial position will correspond to the neuromotor component and the irrefutable result will be that in figure 15c.
As you can see, the 'Neuro Evoked Centric' has re-established the previously lost neuromotor component, due to curarization with a 3 mm shift of the mandible to the right.
- ↑ Rodziewicz TL, Houseman B, Hipskind JE, «Medical Error Reduction and Prevention», StatPearls Publishing LLC, 2022».
PMID:29763131 - ↑
Grandmaison G, Ribordy V, Mancinetti M, «Diagnostic errors : The importance of a systems approach», in Rev Med Suisse, 2021».
PMID:34495586 - ↑ Nikdel C, Nikdel K, Ibarra-Noriega A, Kalenderian A, Walji MF, «Clinical Dental Faculty Members' Perceptions of Diagnostic Errors and How to Avoid Them», in J Dent Educ, 2018».
PMID:29606650
DOI:10.21815/JDE.018.037 - ↑ Amrhein V, Greenland S, McShane B, «Scientists rise up against statistical significance», in Nature, 2019».
PMID:30894741
DOI:10.1038/d41586-019-00857-9 - ↑ Rodgers JL, «The epistemology of mathematical and statistical modeling: a quiet methodological revolution», in Am Psychol, American Psychological Association, 2010, Washington, DC».
PMID:20063905
DOI:10.1037/a0018326 - ↑ Meehl P, «The problem is epistemology, not statistics: replace significance tests by confidence intervals and quantify accuracy of risky numerical predictions», in Am Psychol, American Psychological Association, 1997, Washington, DC».
ISBN: 9781315827353
PMID:20063905
DOI:10.1037/a0018326 - ↑ Sprenger J, Hartmann S, «Bayesian Philosophy of Science. Variations on a Theme by the Reverend Thomas Bayes», Oxford University Press, 2019, Oxford, UK».
ISBN: 9780199672110 - ↑ Wasserstein RL, Schirm AL, Lazar NA, «Moving to a World Beyond “p < 0.05”», in Am Stat, Informa UK Limited, 2019».
ISSN: 1537-2731
DOI:10.1080/00031305.2019.1583913

This is an Open Access resource! - ↑ Dettweiler Ulrich, «The Rationality of Science and the Inevitability of Defining Prior Beliefs in Empirical Research», in Front Psychol, 2019».
PMID:31456724 - PMCID:PMC6700237
DOI:10.3389/fpsyg.2019.01866 - ↑ Boon M, Van Baalen S, «Epistemology for interdisciplinary research - shifting philosophical paradigms of science», in Eur J Philos Sci, 2019. DOI:10.1007/s13194-018-0242-4
- ↑ Boon M, «An engineering paradigm in the biomedical sciences: Knowledge as epistemic tool», in Prog Biophys Mol Biol, 2017.DOI:10.1016/j.pbiomolbio.2017.04.001
- ↑ Codish S, Shiffman RN, «A model of ambiguity and vagueness in clinical practice guideline recommendations», in AMIA Annu Symp Proc, 2005.PMID:16779019
- ↑ Boon M, Van Baalen S, «Epistemology for interdisciplinary research - shifting philosophical paradigms of science», in Eur J Philos Sci, 2019DOI:10.1007/s13194-018-0242-4
- ↑ Boon M, «An engineering paradigm in the biomedical sciences: Knowledge as epistemic tool», in Prog Biophys Mol Biol, 2017DOI:10.1016/j.pbiomolbio.2017.04.001
- ↑ From which to start to finalize the patient orthodontically and prophetically