Difference between revisions of "Encrypted code: Bilateral Motor Evoked Potentials of trigeminal root"
| (10 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{main menu}} | |||
[[File:Meningioma 3 by Gianni Frisardi.jpeg|link=link=Special:FilePath/Meningioma_3_by_Gianni_Frisardi.jpg|alt=|left|frameless]] | [[File:Meningioma 3 by Gianni Frisardi.jpeg|link=link=Special:FilePath/Meningioma_3_by_Gianni_Frisardi.jpg|alt=|left|frameless]] | ||
This detailed summary examines the complex interrelationships between dental malocclusion, postural disorders, and trigeminal neurophysiopathology through the clinical case of a patient known as 'Balancer.' The patient's decade-long suffering from a meningioma at the base of the skull illustrates the challenges and potential misdiagnoses that can occur when traditional dental perspectives are applied without considering deeper neurophysiological issues. The text integrates a broad range of medical insights to argue for a more nuanced approach to diagnosing and treating conditions that straddle neurology and dentistry. | |||
{{ArtBy| | Introduction | ||
The chapter opens by highlighting the limitations of axiomatic assumptions in medical diagnoses, particularly in the complex interplay between dental health and neurological conditions. It introduces the case of 'Balancer,' whose symptoms were initially interpreted within a dental framework but later understood to be indicative of significant neurological pathology. | |||
Trigeminal Neurophysiopathology and Misdiagnosis | |||
The narrative delves into the specifics of trigeminal neurophysiopathology, explaining how the patient's meningioma exerted physical effects on both sensory and motor fibers of the trigeminal nerve system, leading to severe symptoms that were initially misinterpreted as dental issues. The discussion underscores the importance of considering neurophysiological data in dental diagnoses, particularly when patients present with atypical or severe symptoms that do not align with common dental disorders. | |||
Diagnostic Challenges and Electrophysiological Insights | |||
The summary critically evaluates the diagnostic process, emphasizing the role of electrophysiological tests such as the <sub>b</sub>Root-MEPs and assessments of the jaw jerk reflex. These tests revealed the extent of the damage more accurately than dental evaluations and highlighted the need for medical imaging to confirm the presence and impact of the meningioma. | |||
MRI Findings and Neurological Complications | |||
MRI results confirmed the severe implications of the meningioma, showing brainstem displacement and raising urgent questions about the initial stages of the tumor's development. This section reflects on whether earlier detection of the tumor through targeted electrophysiological testing could have altered the patient's treatment trajectory. | |||
Misleading Symptoms and the Importance of Accurate Diagnosis | |||
The patient's case is used to illustrate how symptoms like 'chewing difficulty' can be misleading. The narrative argues for a more integrated diagnostic approach that combines dental and neurological expertise to avoid oversimplified conclusions that may lead to inadequate treatments. | |||
Cognitive Neural Network (CNN) Diagnostic Model | |||
The use of a Cognitive Neural Network (CNN) in diagnosing 'Balancer's' condition is discussed, showcasing how advanced data analysis techniques can aid in distinguishing between symptoms related to dental malocclusions and those stemming from serious neurological conditions. This section details the sequential steps taken through the CNN to refine the diagnosis and better understand the underlying causes of the patient's symptoms. | |||
Clinical Implications and Future Directions | |||
The chapter concludes by discussing the broader clinical implications of the case for both dentistry and neurology. It calls for heightened awareness of the potential for neurological conditions to manifest through symptoms typically associated with dental issues and recommends more interdisciplinary approaches in medical training and practice to prevent similar diagnostic errors. | |||
Summary | |||
This summary not only provides a detailed recount of 'Balancer's' medical journey but also serves as a cautionary tale about the risks of compartmentalized medical thinking. It advocates for a holistic approach to patient care that respects the complex interconnections between different bodily systems and emphasizes the critical importance of accurate, comprehensive diagnostic practices in ensuring effective treatment outcomes.<blockquote> | |||
== Keywords == | |||
'''Trigeminal Neurophysiopathology''' - Refers to the study of diseases that affect the trigeminal nerve, highlighting the nerve's role in conveying sensory information from the face to the brain. This term is crucial for medical content discussing neurological impacts on facial sensation and motor functions. | |||
'''Dental Malocclusion''' - Describes the misalignment of teeth and how they fit together when the jaws are closed. This keyword is key for dental health content, focusing on how teeth alignment affects overall oral health and potentially other bodily functions. | |||
'''Postural Disorders''' - Pertains to conditions that affect the posture or the way the body is positioned when standing or sitting. This term is particularly relevant in discussions about how spinal and muscular health can be influenced by neurological and dental health. | |||
'''Meningioma''' - A type of brain tumor that forms from the meninges, the layers of tissue covering the brain and spinal cord. This keyword is critical for content on brain tumors, discussing symptoms, diagnosis, and treatment options. | |||
'''Electrophysiological Tests''' - Refers to diagnostic tests that measure electrical activity in the body, such as nerve impulses. These tests are crucial in neurology content, especially in diagnosing and understanding the extent of nerve damage. | |||
'''Jaw Jerk Reflex''' - A reflex that helps diagnose disorders of the trigeminal nerve by tapping the jaw and observing the response. This keyword is relevant for neurological examination content, focusing on reflex testing. | |||
'''Cognitive Neural Network (CNN) in Diagnosis''' - Discusses the application of advanced data analysis techniques in medical diagnostics, especially for integrating and analyzing patient data for better diagnostic accuracy. This term is significant for content on medical technology and innovations in diagnostics. | |||
'''MRI Findings in Neurology''' - MRI (Magnetic Resonance Imaging) findings that provide insights into brain and nerve conditions, essential for content related to medical imaging techniques and their applications in diagnosing neurological disorders. | |||
'''Motor Evoked Potentials (MEPs)''' - A diagnostic measure of the electrical activity in response to stimulation of the motor cortex, used to assess the functionality of motor pathways, particularly relevant for neurophysiological testing content. | |||
'''Neurological and Dental Integration''' - Focuses on the interdisciplinary approach between neurology and dentistry to tackle complex cases that exhibit symptoms affecting both the neurological and dental systems, crucial for content on comprehensive patient care and diagnostic strategies.</blockquote>{{ArtBy| | |||
| autore = Gianni Frisardi | | autore = Gianni Frisardi | ||
| autore2 = Giorgio Cruccu | | autore2 = Giorgio Cruccu | ||
| Line 23: | Line 53: | ||
| autore5 = | | autore5 = | ||
| autore6 = | | autore6 = | ||
| | | }} | ||
===Introduction=== | ===Introduction=== | ||
In the introductory chapter concerning the 3rd clinical case affected by meningioma in which the masticatory difficulty reported by the patient 'Balancer' had been correlated to a prosthetic rehabilitation discrepancy, we have already arrived at a first diagnostic filter considering the neurological assertion to be valid than the dental one. Consequently, one can concentrate on intercepting the tests necessary to decrypt the machine language code that the CNS sends out converted into verbal language. Apparently this verbal language would address the case in a Postural disorder related to a dental malocclusion due to incongruous prosthetic rehabilitation. If, on the one hand, there may be an asymmetry of the interferential EMG of the masseters due to a prosthetic occlusal imbalance, on the other, such an evident asymmetry of the jaw jerk and the silent period cannot be justified. For this reason, it is essential to continue with the Masticationpedia diagnostic model in order to arrive at an exact and rapid conclusive diagnosis. We therefore begin with the 'Cognitive Neural Network' which responds, as we know by now, with a sequence of scientific-clinical data, always taking into consideration the importance of the 'initiation' step which in this case has been set in 'Gait'. | |||
<blockquote> | |||
<math>CNN=\sum ( </math> [https://pubmed.ncbi.nlm.nih.gov/?term=%27gait+%27&filter=datesearch.y_10&size=200 Gait] (45.300), [https://pubmed.ncbi.nlm.nih.gov/?term=%27gait+AND+motor+evoked+potentials+%27&filter=datesearch.y_10&size=200 motor evoked potentials] (231),[https://pubmed.ncbi.nlm.nih.gov/?term=%27gait+AND+motor+evoked+potentials+AND+reflex%27&filter=datesearch.y_10&size=200 reflex] (36), [https://pubmed.ncbi.nlm.nih.gov/29696497/ jaw](1) <math>\longrightarrow</math> 'Cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS) with chronic cough and preserved muscle stretch reflexes: evidence for selective sparing of afferent Ia fibres'</blockquote> | <math>CNN=\sum ( </math> [https://pubmed.ncbi.nlm.nih.gov/?term=%27gait+%27&filter=datesearch.y_10&size=200 Gait] (45.300), [https://pubmed.ncbi.nlm.nih.gov/?term=%27gait+AND+motor+evoked+potentials+%27&filter=datesearch.y_10&size=200 motor evoked potentials] (231),[https://pubmed.ncbi.nlm.nih.gov/?term=%27gait+AND+motor+evoked+potentials+AND+reflex%27&filter=datesearch.y_10&size=200 reflex] (36), [https://pubmed.ncbi.nlm.nih.gov/29696497/ jaw](1) <math>\longrightarrow</math> 'Cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS) with chronic cough and preserved muscle stretch reflexes: evidence for selective sparing of afferent Ia fibres'</blockquote> | ||
=== | ===Diagnostic sequence === | ||
====1st Step: CNN Sequence==== | ====1st Step: CNN Sequence ==== | ||
* | *'''''<math>\tau</math>''' Coherence Demarcator:'' As we have previously described for the other clinical cases, the first step is an initialization command of the Cognitive Neural Network 'CNN' which derives, in fact, from a previous cognitive elaboration on the assertions in the dental and neurological context in which the ' Demarcator of Consistency' gave a prevailing weight. The dental context has already been eliminated from the Consistency Demarcator. From what emerges from the neurological statements, the 'State' of the Trigeminal Nervous System' appears to be strongly damaged. The initialization command will therefore be 'Gait'. | ||
===== | * 1st loop open: The first result of the 'CNN' for the keyword '[https://pubmed.ncbi.nlm.nih.gov/?term=%27gait++%27&filter=datesearch.y_10&ac=yes&cauthor_id=None&user_filter=&schema=none&page=1&whatsnew=None&show_snippets=on&format=summary&sort=relevance&sort_order=desc&size=200 Gait]' returns 45,300 results, obviously, too vast to be exhaustive but having ascertained in the context analysis phase a serious trigeminal electrophysiological situation with marked structural anomalies and functional, we can safely enter a correlated key such as ' Motor Evoked Potentials' without specifying the trigeminal district which could encroach on the identified set. | ||
*2st loop open: To this second query '[https://pubmed.ncbi.nlm.nih.gov/?term=%27gait+AND+motor+evoked+potentials+%27&filter=datesearch.y_10&size=200 Motor Evoked Potentials]' the database replies with 231 results that are still too vast as an answer and therefore we are looking for a key more similar to the clinical case presented. Since the most anomalous results in the neurological context have emerged from the latency and amplitude alterations of the trigeminal reflexes, an appropriate access key could be, in fact, 'Reflex' also without specifying 'trigeminal' for the same anticipated reasons. | |||
*3st loop open: To the '[https://pubmed.ncbi.nlm.nih.gov/?term=%27gait+AND+motor+evoked+potentials+AND+reflex%27&filter=datesearch.y_10&size=200 Reflex]'request, the response was 36 results which narrowed the field of analysis for the diagnosis of our patient 'Balancer'. Only at this level of the CNN can one attempt to close the loop with a more specific request such as 'Jaw'. In this way we have not lost contact with the whole considered and we have remained in the field of electrophysiology. | |||
*4st loop open: The request '[https://pubmed.ncbi.nlm.nih.gov/29696497/ jaw]' in fact in the 36 results it is possible to intercept an article in which some electrophysiological parameters are reported which correspond to a clinical situation of cerebellar ataxia, a pathology in which postural and gait instability is a clinical sign impressive and important. | |||
<nowiki/><nowiki/> | |||
=====2st Step: CNN analysis ===== | |||
The 'CNN' loop closure analy of course is based on the terminal article which basically describe five patients with cerebellar ataxia, neuropathy and vestibular areflexia syndrome (CANVAS) with chronic cough and lower limb muscle stretch reflexes preserve yourself.<ref name=":0">Jon Infante, Antonio García, Karla M Serrano-Cárdenas, Rocío González-Aguado, José Gazulla, Enrique M de Lucas, José Berciano. Cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS) with chronic cough and preserved muscle stretch reflexes: evidence for selective sparing of afferent Ia fibres.J Neurol . 2018 Jun;265(6):1454-1462. doi: 10.1007/s00415-018-8872-1.Epub 2018 Apr 25. | |||
</ref> In particular, somatosensory evoked potentials were absent or severely attenuated. Biceps and hamstring T-reflex recordings were normal, while the masseter reflex was absent or attenuated.<blockquote>[[File:Meningioma 2 by Gianni Frisardi.jpeg|link=link=Special:FilePath/Meningioma_2_by_Gianni_Frisardi.jpg|alt=|thumb|'''Figure 1:''' Neurological statement highlighting a severe right jaw jerk latency and amplitude abnormality]]The first observation to be made is that the patients were suffering from chronic spasmodic cough and the second observation was the preservation of the tendon reflexes of the lower limbs. In our patient 'Balancer', on the other hand, there was a total absence of the mandibular tendon reflex<ref>The history of examination of reflexes. Boes CJ.J Neurol. 2014 Dec;261(12):2264-74. doi: 10.1007/s00415-014-7326-7. Epub 2014 Apr 3.PMID: 24695995 </ref> (<math>\gamma_1</math>) so that the neurological damage was very evident at the trigeminal midbrain level. (Figure 1) The multifunctional contribution of the midbrain synaptic circuitry by the proprioceptive nerve endings ( <math>1a</math> e <math>\gamma</math>) are of primary importance both for posture and for cervico-oculomotor reflexes. A very interesting article by Yongmei Chen et al.<ref>Chen Y, Gong X, Ibrahim SIA, Liang H, Zhang J.. Convergent innervations of mesencephalic trigeminal and vestibular nuclei neurons onto oculomotor and pre-oculomotor neurons-Tract tracing and triple labeling in rats. PLoS One. 2022 Nov 28;17(11):e0278205. doi: 10.1371/journal.pone.0278205. eCollection 2022.PMID: 36441755 </ref> showed, through markers, how neurons afferent to the trigeminal mesencephalic nucleus (Vme) from the jaw muscles project to the oculomotor nuclei (III/IV) and their premotor neurons in the interstitial nucleus of Cajal (INC), a well-known pre-oculomotor center that vertically manipulates torsional eye movements. | |||
The conceptual conclusion of the authors was that the Vme proprioceptive neurons of the masticatory projecting muscles at III/IV and INC would detect spindle activity to spatial changes of the jaw conditioned by the force of gravity and/or by the connection between the mandible during rotation of the head. Thus, the convergent innervation of Vme and MVN neurons on the oculomotor and pre-oculomotor nuclei would be a neuroanatomical substrate for the interaction of masticatory proprioception with vestibulo-ocular signals on the oculomotor system during vertical-torsional VOR. The contribution of this article obviously allows us to consider a correlation between the trigeminal system, posture and gait, therefore, the abnormal asymmetry of the jaw jerk could be related to a postural disorder of our patient 'Balancer' | |||
</blockquote> | |||
But there is also to consider the article of Jon Infante <ref name=":0" /> highlighted that all five patients were in the seventh decade of age, their gait imbalance having started in the fifth decade. In four patients, cough preceded gait imbalance between 15 and 29 years of age; the cough was spasmodic and triggered by variable factors. In addition, vestibular function tests showed bilateral impairment of the vestibulo-ocular reflex. <blockquote>[[File:Meningioma 6 by Gianni Frisardi.jpeg|link=link=Special:FilePath/Meningioma_6_by_Gianni_Frisardi.jpg|alt=|thumb|'''Figure 2:''' Occlusal aspect of the 'Balancer' patient who had the occlusal incongruity on the right side restored several times.]] | |||
The presence of chronic spasmodic cough, in this study, for over 10 years even before balance and postural disturbances showed up, suggest that machine language, as repeatedly exposed in the specific chapters of Masticationpedia, is a reality not to be overlooked because the ambiguous and vague verbal language covers the information of the encrypted code. As we will demonstrate in the course of the discussion, the analog of the spasmodic cough symptom of the patients reported by Jon Infante's article could be the repeated reporting to the dental colleagues of the chewing difficulty by our patient 'Balancer'. (Figure 2) This parameter has not been considered as an 'encrypted code' but only an element of verbal language logic and therefore vague and ambiguous. The continuous remaking of the prosthetic rehabilitation dampened even more the information of the machine language until the temporal and spatial addition of the organic damage was transformed<ref name=":0" /> into a macroscopic symptom of vertigo and loss of balance in walking </blockquote> | |||
</ | Jon Infante's article<ref name=":0" /> concludes with a striking statement, i.e. that '''spasmodic cough''' can be an integral part of the clinical picture in CANVAS, anticipating the appearance of postural imbalance by several decades and ''that sparing of muscle spindle afferents (Ia fibers) is probably the pathophysiological basis of normoreflexia.'' | ||
{{Q2|We came to the conclusion that the patient's postural disorder could not be related to the rehabilitative occlusal incongruity but to a neurological damage but the question now is the following:|........is the neurological damage functional or organic?}} | |||
=== | === Decryption process === | ||
The diagnostic procedure followed routinely according to the Masticationpedia model has allowed us to eliminate, through the coherence demarcator, the dental context to follow the neurological one and to deepen through the 'Cognitive Neural Network' (CNN) the possible correlations between symptoms and neurophysiological abnormalities in patients with postural and walking disorders due to functional pathologies (labyrinthitis, neuropathies, etc.) from organic ones (tumors, demyelinations, etc.). Now we must try to decrypt the encrypted message of the machine language of the Trigeminal Nervous System. | |||
==== | ====Encrypted code==== | ||
[[File:Ortognatica Jaw jerk.jpg|link=link=Special:FilePath/Ortognatica_Jaw_jerk.jpeg|alt=|thumb|''' | [[File:Ortognatica Jaw jerk.jpg|link=link=Special:FilePath/Ortognatica_Jaw_jerk.jpeg|alt=|thumb|'''Figure 2:''' Determination of the functional component of the Central Nervous System. The results for patient 2 (normocclusion) show an area of 1.37 mV/ms and 0.13 mV/ms on the right and left masseter, respectively. This shows an asymmetry between sides of about 100%.]][[File:Meningioma 2 by Gianni Frisardi.jpeg|link=link=Special:FilePath/Meningioma_2_by_Gianni_Frisardi.jpg|alt=|thumb|'''Figure 1:''' Neurological statments <math>\gamma_1</math> highlighting severe jaw jerk latency abnormality |left]] | ||
As anticipated, first of all we were able to highlight a serious absence of the jaw jerk reported as <math>\gamma_1=1\longrightarrow</math> Abnormality, positive report (Figure 1) but as already mentioned in the chapter | |||
' [[Conclusions on the status quo in the logic of medical language regarding the masticatory system]]' also in the patient treated with orthognathic surgery we were able to detect an absence of the jaw jerk (figure 2) restored immediately after evoked neurognathological rehabilitation. In our case 'Balancer' we have an additional objective disorder that of masticatory difficulty and together with the postural disorder there were nystagmus and vertigo. | |||
===== | A further assertion in favor of organic damage was also the presence of a latency delay on the right side of the electrical silent period, <math>\gamma_3=1\longrightarrow</math> Abnormality, positivity of the report, which suggests a slowing of the nerve conduction speed. In this instance we cannot say whether the delay refers to damage to the sensory or motor fibers until we approach the study of the nerve conduction of the motor trigeminal roots. | ||
[[File:Meningioma 5 by Gianni Frisardi.jpeg|link=link=Special:FilePath/Meningioma_5_by_Gianni_Frisardi.jpg|alt=|300x300px|thumb|''' | =====Motor evoked potentials of the trigeminal root===== | ||
[[File:Meningioma 5 by Gianni Frisardi.jpeg|link=link=Special:FilePath/Meningioma_5_by_Gianni_Frisardi.jpg|alt=|300x300px|thumb|'''Figure 4:''' MRI report of meningioma in right skull base]][[File:Meningioma 3 by Gianni Frisardi.jpeg|thumb|'''Figure 3:''' Bilateral transcranial electrical stimulation evoked responses. A marked asymmetry of amplitude in the right Masseter is evident.|alt=|left]] | |||
In our masticatory neurophysiology laboratory we have developed a technique of electrical transcranial electrostimulation of the two trigeminal roots simultaneously and synchronized with the electrical stimulus. In the various chapters already published some technical information on the method is reported but we intend to expose them exhaustively in the section 'Extraordinary science'. In this context we can only consider and confirm a significant amplitude asymmetry of the motor evoked responses as shown in figure 3. The markers 1A and 2A indicate the latency which, unlike the silent period, is symmetrical and this data confirms the structural damage of the sensory fibers including those proprioceptive from masticatory muscles. At this point we can not only confirm and justify the neurological choice of the diagnostic context but also conclude with a pre-diagnosis of cerebellar neurological damage with involvement of the trigeminal mesencephalic axis. | |||
The Magnetic Resonance of the brain, unfortunately, solves our doubts with a report of solid expansive lesion with mass effect in the right hemisphere, it is not clear whether it has a supra or sub tentorial origin, it certainly determines compressive phenomena on the midbrain - trunk and on the fourth ventricle with dilatation of the cisternae and ventricles upstream. That it is a meningioma is very likely because he has no perilesional edema.<center></center> | |||
==='''Final considerations'''=== | ==='''Final considerations'''=== | ||
We summarize the clinical diagnostic path following the Masticationpedia model so that the latter can be considered a fluid and dynamic process to reach a diagnostic target in the fastest and most detailed way. | |||
# | # Context analysis through dental and neurological laboratory tests | ||
# | #Choice of neurological statement filtered by the '''''<math>\tau</math>''''' ''Coherence Demarcator'' | ||
# | # Evaluation of the clinical case in the Cognitive Neural Network (CNN) | ||
# | #Closing the CNN loop with Jon Infante's article<ref name=":0" /> and the consideration of the organic/functional damage of our patient's trigeminal sensory-motor structures through the observation of the amplitude asymmetry of the 'bRoot-MEPs'. The logical sequence of the tests carried out with the numbering restored has been ordered in the image gallery. | ||
<Center> | <Center> | ||
<gallery widths="340" heights="300" perrow="2" slideshow""=""> | <gallery widths="340" heights="300" perrow="2" slideshow""=""> | ||
File:Meningioma 3 by Gianni Frisardi.jpeg|''' | File:Meningioma 3 by Gianni Frisardi.jpeg|'''Figure 1a:''' The first test that must always be performed in complex clinical cases is, in fact, the <sub>b</sub>Root-MEPs | ||
File:Meningioma 2 by Gianni Frisardi.jpeg|''' | File:Meningioma 2 by Gianni Frisardi.jpeg|'''Figure 1b:''' The second test is the jaw jerk which returns a sort of analysis of the integrity of the midbrain system. In our case 'Balancer' an abnormal asymmetry is evident to the detriment of the right masseter | ||
File:Meningioma 4 by Gianni Frisardi.jpeg|''' | File:Meningioma 4 by Gianni Frisardi.jpeg|'''Figure 1c:''' After verifying the level of integrity of the midbrain area through tests involving monosynaptic reflexes such as jaw jerk, the level of complexity is raised by evoking the electrical silent period which is a polysynaptic reflex. The latency delay on the right masseter is evident | ||
File:Meningioma 5 by Gianni Frisardi.jpeg|''' | File:Meningioma 5 by Gianni Frisardi.jpeg|'''Figure 1d:''' Obviously after these results, the patient cannot be considered affected by postural disorder but by organic neurological pathology and the Nuclear Magnetic Resonance of the brain shows it in all its diagnostic potential. | ||
</gallery> | </gallery> | ||
</Center> | </Center> | ||
=== | ===Conclusion=== | ||
We now have evidence of both direct and indirect functional organic correlation between the trigeminal system and the vestibular system, just think of the study of mVEMP (Vestibular Evoked Myogenic Potentials) now recognized as a solid and reliable test for assessing the functional integrity of the reflex pathway vestibulo-masseteric<ref>Sangu Srinivasan Vignesh, Niraj Kumar Singh, Krishna Rajalakshmi. Tone Burst Masseter Vestibular Evoked Myogenic Potentials: Normative Values and Test-Retest Reliability. J Am Acad Audiol. 2021 May;32(5):308-314. doi: 10.1055/s-0041-1728718.Epub 2021 Jun 1. | |||
</ref> in clinical manifestations with involvement of the trigeminal and vestibular system as in schwannomas<ref>Ashutosh Kumar, Sanjay Behari, Jayesh Sardhara, Prabhaker Mishra, Vivek Singh, Vandan Raiyani, Kamlesh Singh Bhaisora, Arun Kumar Srivastava . Quantitative assessment of brainstem distortion in vestibular schwannoma and its implication in occurrence of hydrocephalus.Br J Neurosurg . 2022 Dec;36(6):686-692. doi: 10.1080/02688697.2022.2047155.Epub 2022 Mar 7. | |||
</ref><ref>Daniel Moualed, Jonathan Wong, Owen Thomas, Calvin Heal, Rukhtam Saqib, Cameron Choi, Simon Lloyd, Scott Rutherford, Emma Stapleton, Charlotte Hammerbeck-Ward, Omar Pathmanaban, Roger Laitt, Miriam Smith, Andrew Wallace, Mark Kellett, Gareth Evans, Andrew King, Simon Freeman. Prevalence and natural history of schwannomas in neurofibromatosis type 2 (NF2): the influence of pathogenic variants. Eur J Hum Genet. 2022 Apr;30(4):458-464. doi: 10.1038/s41431-021-01029-y.Epub 2022 Jan 24. | |||
</ref> or in the presence of acoustic neuromas<ref>Claudia Cassandro, Roberto Albera, Luca Debiasi, Andrea Albera, Ettore Cassandro, Alfonso Scarpa, Massimo Ralli. What factors influence treatment decision making in acoustic neuroma? Our experience on 103 cases. Int Tinnitus J. 2020 Nov 18;24(1):21-25.doi: 10.5935/0946-5448.20200004. | |||
</ref> as much as the relative correlation between dental occlusion and the vestibular system but this does not allow, given the seriousness of the diagnostic error that it would result, to consider this last clinical condition a clinically validated scientific datum. In the Appendix an example of what might happen. | |||
This last assertion, perhaps risky because it is controversial, collides with the evidence of a striking fact highlighted several times during the drafting of the chapters of Masticationpedia, that of machine language and verbal language. A vague and ambiguous verbal language can generate scientific convictions depending on how it is proposed but in substance it covers and hides a much more decisive and formal machine language. For example, the verbal language deduced that the postural disturbances of the 'Balancer' patient were caused by an incongruous prosthetic rehabilitation while the machine language signaled an organic sensorineural deficit (absence of the jaw jerk, latency delays of the silent period, large reduction in the amplitude of the <sub>b</sub>Root-MEPs. | |||
The lack of information on the velocity and the mandibular position at the midbrain level, in fact, determines an incapacity of stereognostic awareness in which the patient does not recognize the spatial and temporal position of the mandible. The decrease in the recruitment of the motor units of the masticatory muscles and not only of the tested masseter with an obvious decrease in the masticatory force is the result of this organic and functional damage. All this indicates an impairment of the proprioceptive territory but we do not know if the sensory structures have also been involved. The electrical silent period, on the other hand, shows a severe delay in latency with a slowing of nerve conduction velocity. To conclude the neurophysiopathological diagnostic picture is the observation that the right trigeminal motor root has lost most of its motor fibers. | |||
< | However, it should be noted that in such a serious clinical condition we see a decrease in the amplitude of the <sub>b</sub>Root-MEPs but not a latency asymmetry. This finding indicates that there was direct damage to the trigeminal motor fibers from tumor compression (axonotmesis) but not demyelination (neuropraxia) which would have shown latency delay on the right masseter. It is advisable to briefly describe the definition of neurological damage bearing in mind that the equivalent of the spinal peripheral nerve for the trigeminal nervous system corresponds to the motor trigeminal root. | ||
'''Neurotmesis''' is caused by a transection of a nerve and is the worst degree of peripheral nerve injury. In neurotmesis, the entire nerve, including the endoneurium, perineurium, and epineurium, is completely severed. Neurotmesis leads to disruption of the axon, myelin sheath, and connective tissues. The prognosis for spontaneous recovery is poor without surgery.<ref>Kaya Y, Sarikcioglu L. Sir Herbert Seddon (1903-1977) and his classification scheme for peripheral nerve injury. Childs Nerv Syst. 2015 Feb;31(2):177-80. </ref> Sunderland's fifth-degree lesion fits the definition of neurotmesis in the Seddon classification and represents the highest degree of nerve injury, with a complete nerve defect. | |||
'''Neurapraxia''' is a nerve injury commonly induced by focal demyelination and/or ischemia and is the mildest type of peripheral nerve injury. In neurapraxia, nerve impulse conduction is blocked in the injured area, sensory and motor connection is lost, but all morphologic structures of the nerve stump, including the endoneurium, perineurium, and epineurium, remain intact. | |||
'''Axonotmesis''' is a relatively more serious type of peripheral nerve injury and is usually caused by crushing, stretching, or percussion. In axonotmesis, the epineurium is intact, while the perineurium and endoneurium may be disrupted. The axon is separated from the soma and the axon and myelin sheath are disrupted. Wallerian degeneration occurs in the axon stump distal to the injury site within 24 to 36 hours after peripheral nerve injury. | |||
After neurotmesis, Schwann cells respond adaptively to axonal disruption, transitioning from a highly myelinated state to a dedifferentiated state. De-differentiated Schwann cells engulf axons and myelin debris and form a regenerative pathway for axon outgrowth. Additionally, activated Schwann cells secrete a group of cytokines, including tumor necrosis factor-alpha, interleukin-1 alpha, and leukemia inhibitory factor, to recruit macrophages and facilitate digestion of debris. Schwann cells also secrete a group of neurotrophic factors, including nerve growth factor, brain-derived neurotrophic factor, and glial cell line-derived neurotrophic factor, to encourage neuron survival and axon elongation.<ref>Jessen KR, Mirsky R, Lloyd AC. Schwann Cells: Development and Role in Nerve Repair. Cold Spring Harb Perspect Biol. 2015 May 08;7(7):a020487. </ref><ref>Madduri S, Gander B. Schwann cell delivery of neurotrophic factors for peripheral nerve regeneration. J Peripher Nerv Syst. 2010 Jun;15(2):93-103.</ref><ref>Yi S, Zhang Y, Gu X, Huang L, Zhang K, Qian T, Gu X. Application of stem cells in peripheral nerve regeneration. Burns Trauma. 2020;8:tkaa002</ref> | |||
Needle electromyography (EMG) is the most sensitive electrodiagnostic study for motor axon loss, and low-amplitude motor responses appear with severe injuries. Decrease in motor response amplitude begins around days 2-3 and is complete by day 6. This reflects the fact that neuromuscular junction degeneration precedes axon degeneration and motor responses are dependent on neuromuscular junction transmission.<ref>Ferrante MA. The Assessment and Management of Peripheral Nerve Trauma. Curr Treat Options Neurol. 2018 Jun 01;20(7):25.</ref> | |||
===Appendix=== | |||
Patient treated by a dental colleague for a prosthetic rehabilitation following postural methods which indicated the best Centric occlusion through dynamometric platforms. The patient came to our observation presenting a clinical state of fasciculation of the masseter muscles as well as, obviously, an occlusal and masticatory discomfort. The centric position finalized by the colleague was, therefore, correlated with the best postural dynamometry response but unfortunately this did not result. | |||
Observing figures 5,6 and 7 we can understand how axioms are built that do not respond to a validated scientific criterion, much less to a biological reality. Thinking that a remote phenomenon such as postural stability dictated by a dynamometric platform can validate the choice of a position occlusal achieved manually by the operator breaks down on the observation that by observing the state of the trigeminal system by measuring it through a demand (<sub>b</sub>Root-MEPs) the system responds with its own spatial position not dictated by posturological correlation nor by the manual maneuvers of the operator but by its own vectorial neuromotor result.<center> | |||
<gallery widths="260" heights="300" perrow="3" slideshow""=""> | |||
<center> | File:Pz.posture.png|'''Figure 5:''' Rehabilitated patient following posturological indications from dynamometry data. | ||
<gallery widths=" | File:Pre Root-MEPs.jpeg|'''Figure 6:''' Centric occlusion defined through data indications of the dynamometric platform. | ||
File:Pz.posture.png|''' | File:Post Root-MEPs.jpeg|'''Figure 7:''' Centric position resulting from bRoot-MEPs. Note the retrusion of at least 3mm and the leftward displacement of the mandible. | ||
File:Pre Root-MEPs.jpeg|''' | |||
File:Post Root-MEPs.jpeg|''' | |||
</gallery> | </gallery> | ||
</center>{{Q2|In | </center> | ||
{{Q2|In conclusion, the correlation between the vestibular and trigeminal systems, although present from a neurophysiopathological point of view, should not be considered a clinical procedure in masticatory rehabilitation.|….should only be considered as an experimental exploratory field to deduce more knowledge on neuronal connectivity.}} | |||
Revision as of 13:13, 12 May 2024
Encrypted code: Bilateral Motor Evoked Potentials of trigeminal root

This detailed summary examines the complex interrelationships between dental malocclusion, postural disorders, and trigeminal neurophysiopathology through the clinical case of a patient known as 'Balancer.' The patient's decade-long suffering from a meningioma at the base of the skull illustrates the challenges and potential misdiagnoses that can occur when traditional dental perspectives are applied without considering deeper neurophysiological issues. The text integrates a broad range of medical insights to argue for a more nuanced approach to diagnosing and treating conditions that straddle neurology and dentistry.
Introduction The chapter opens by highlighting the limitations of axiomatic assumptions in medical diagnoses, particularly in the complex interplay between dental health and neurological conditions. It introduces the case of 'Balancer,' whose symptoms were initially interpreted within a dental framework but later understood to be indicative of significant neurological pathology.
Trigeminal Neurophysiopathology and Misdiagnosis The narrative delves into the specifics of trigeminal neurophysiopathology, explaining how the patient's meningioma exerted physical effects on both sensory and motor fibers of the trigeminal nerve system, leading to severe symptoms that were initially misinterpreted as dental issues. The discussion underscores the importance of considering neurophysiological data in dental diagnoses, particularly when patients present with atypical or severe symptoms that do not align with common dental disorders.
Diagnostic Challenges and Electrophysiological Insights The summary critically evaluates the diagnostic process, emphasizing the role of electrophysiological tests such as the bRoot-MEPs and assessments of the jaw jerk reflex. These tests revealed the extent of the damage more accurately than dental evaluations and highlighted the need for medical imaging to confirm the presence and impact of the meningioma.
MRI Findings and Neurological Complications MRI results confirmed the severe implications of the meningioma, showing brainstem displacement and raising urgent questions about the initial stages of the tumor's development. This section reflects on whether earlier detection of the tumor through targeted electrophysiological testing could have altered the patient's treatment trajectory.
Misleading Symptoms and the Importance of Accurate Diagnosis The patient's case is used to illustrate how symptoms like 'chewing difficulty' can be misleading. The narrative argues for a more integrated diagnostic approach that combines dental and neurological expertise to avoid oversimplified conclusions that may lead to inadequate treatments.
Cognitive Neural Network (CNN) Diagnostic Model The use of a Cognitive Neural Network (CNN) in diagnosing 'Balancer's' condition is discussed, showcasing how advanced data analysis techniques can aid in distinguishing between symptoms related to dental malocclusions and those stemming from serious neurological conditions. This section details the sequential steps taken through the CNN to refine the diagnosis and better understand the underlying causes of the patient's symptoms.
Clinical Implications and Future Directions The chapter concludes by discussing the broader clinical implications of the case for both dentistry and neurology. It calls for heightened awareness of the potential for neurological conditions to manifest through symptoms typically associated with dental issues and recommends more interdisciplinary approaches in medical training and practice to prevent similar diagnostic errors.
Summary
This summary not only provides a detailed recount of 'Balancer's' medical journey but also serves as a cautionary tale about the risks of compartmentalized medical thinking. It advocates for a holistic approach to patient care that respects the complex interconnections between different bodily systems and emphasizes the critical importance of accurate, comprehensive diagnostic practices in ensuring effective treatment outcomes.
Keywords
Trigeminal Neurophysiopathology - Refers to the study of diseases that affect the trigeminal nerve, highlighting the nerve's role in conveying sensory information from the face to the brain. This term is crucial for medical content discussing neurological impacts on facial sensation and motor functions.
Dental Malocclusion - Describes the misalignment of teeth and how they fit together when the jaws are closed. This keyword is key for dental health content, focusing on how teeth alignment affects overall oral health and potentially other bodily functions.
Postural Disorders - Pertains to conditions that affect the posture or the way the body is positioned when standing or sitting. This term is particularly relevant in discussions about how spinal and muscular health can be influenced by neurological and dental health.
Meningioma - A type of brain tumor that forms from the meninges, the layers of tissue covering the brain and spinal cord. This keyword is critical for content on brain tumors, discussing symptoms, diagnosis, and treatment options.
Electrophysiological Tests - Refers to diagnostic tests that measure electrical activity in the body, such as nerve impulses. These tests are crucial in neurology content, especially in diagnosing and understanding the extent of nerve damage.
Jaw Jerk Reflex - A reflex that helps diagnose disorders of the trigeminal nerve by tapping the jaw and observing the response. This keyword is relevant for neurological examination content, focusing on reflex testing.
Cognitive Neural Network (CNN) in Diagnosis - Discusses the application of advanced data analysis techniques in medical diagnostics, especially for integrating and analyzing patient data for better diagnostic accuracy. This term is significant for content on medical technology and innovations in diagnostics.
MRI Findings in Neurology - MRI (Magnetic Resonance Imaging) findings that provide insights into brain and nerve conditions, essential for content related to medical imaging techniques and their applications in diagnosing neurological disorders.
Motor Evoked Potentials (MEPs) - A diagnostic measure of the electrical activity in response to stimulation of the motor cortex, used to assess the functionality of motor pathways, particularly relevant for neurophysiological testing content.
Neurological and Dental Integration - Focuses on the interdisciplinary approach between neurology and dentistry to tackle complex cases that exhibit symptoms affecting both the neurological and dental systems, crucial for content on comprehensive patient care and diagnostic strategies.
Introduction
In the introductory chapter concerning the 3rd clinical case affected by meningioma in which the masticatory difficulty reported by the patient 'Balancer' had been correlated to a prosthetic rehabilitation discrepancy, we have already arrived at a first diagnostic filter considering the neurological assertion to be valid than the dental one. Consequently, one can concentrate on intercepting the tests necessary to decrypt the machine language code that the CNS sends out converted into verbal language. Apparently this verbal language would address the case in a Postural disorder related to a dental malocclusion due to incongruous prosthetic rehabilitation. If, on the one hand, there may be an asymmetry of the interferential EMG of the masseters due to a prosthetic occlusal imbalance, on the other, such an evident asymmetry of the jaw jerk and the silent period cannot be justified. For this reason, it is essential to continue with the Masticationpedia diagnostic model in order to arrive at an exact and rapid conclusive diagnosis. We therefore begin with the 'Cognitive Neural Network' which responds, as we know by now, with a sequence of scientific-clinical data, always taking into consideration the importance of the 'initiation' step which in this case has been set in 'Gait'.
Gait (45.300), motor evoked potentials (231),reflex (36), jaw(1) 'Cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS) with chronic cough and preserved muscle stretch reflexes: evidence for selective sparing of afferent Ia fibres'


Diagnostic sequence
1st Step: CNN Sequence
- Coherence Demarcator: As we have previously described for the other clinical cases, the first step is an initialization command of the Cognitive Neural Network 'CNN' which derives, in fact, from a previous cognitive elaboration on the assertions in the dental and neurological context in which the ' Demarcator of Consistency' gave a prevailing weight. The dental context has already been eliminated from the Consistency Demarcator. From what emerges from the neurological statements, the 'State' of the Trigeminal Nervous System' appears to be strongly damaged. The initialization command will therefore be 'Gait'.

- 1st loop open: The first result of the 'CNN' for the keyword 'Gait' returns 45,300 results, obviously, too vast to be exhaustive but having ascertained in the context analysis phase a serious trigeminal electrophysiological situation with marked structural anomalies and functional, we can safely enter a correlated key such as ' Motor Evoked Potentials' without specifying the trigeminal district which could encroach on the identified set.
- 2st loop open: To this second query 'Motor Evoked Potentials' the database replies with 231 results that are still too vast as an answer and therefore we are looking for a key more similar to the clinical case presented. Since the most anomalous results in the neurological context have emerged from the latency and amplitude alterations of the trigeminal reflexes, an appropriate access key could be, in fact, 'Reflex' also without specifying 'trigeminal' for the same anticipated reasons.
- 3st loop open: To the 'Reflex'request, the response was 36 results which narrowed the field of analysis for the diagnosis of our patient 'Balancer'. Only at this level of the CNN can one attempt to close the loop with a more specific request such as 'Jaw'. In this way we have not lost contact with the whole considered and we have remained in the field of electrophysiology.
- 4st loop open: The request 'jaw' in fact in the 36 results it is possible to intercept an article in which some electrophysiological parameters are reported which correspond to a clinical situation of cerebellar ataxia, a pathology in which postural and gait instability is a clinical sign impressive and important.
2st Step: CNN analysis
The 'CNN' loop closure analy of course is based on the terminal article which basically describe five patients with cerebellar ataxia, neuropathy and vestibular areflexia syndrome (CANVAS) with chronic cough and lower limb muscle stretch reflexes preserve yourself.[1] In particular, somatosensory evoked potentials were absent or severely attenuated. Biceps and hamstring T-reflex recordings were normal, while the masseter reflex was absent or attenuated.
The first observation to be made is that the patients were suffering from chronic spasmodic cough and the second observation was the preservation of the tendon reflexes of the lower limbs. In our patient 'Balancer', on the other hand, there was a total absence of the mandibular tendon reflex[2] () so that the neurological damage was very evident at the trigeminal midbrain level. (Figure 1) The multifunctional contribution of the midbrain synaptic circuitry by the proprioceptive nerve endings ( e ) are of primary importance both for posture and for cervico-oculomotor reflexes. A very interesting article by Yongmei Chen et al.[3] showed, through markers, how neurons afferent to the trigeminal mesencephalic nucleus (Vme) from the jaw muscles project to the oculomotor nuclei (III/IV) and their premotor neurons in the interstitial nucleus of Cajal (INC), a well-known pre-oculomotor center that vertically manipulates torsional eye movements.
The conceptual conclusion of the authors was that the Vme proprioceptive neurons of the masticatory projecting muscles at III/IV and INC would detect spindle activity to spatial changes of the jaw conditioned by the force of gravity and/or by the connection between the mandible during rotation of the head. Thus, the convergent innervation of Vme and MVN neurons on the oculomotor and pre-oculomotor nuclei would be a neuroanatomical substrate for the interaction of masticatory proprioception with vestibulo-ocular signals on the oculomotor system during vertical-torsional VOR. The contribution of this article obviously allows us to consider a correlation between the trigeminal system, posture and gait, therefore, the abnormal asymmetry of the jaw jerk could be related to a postural disorder of our patient 'Balancer'




But there is also to consider the article of Jon Infante [1] highlighted that all five patients were in the seventh decade of age, their gait imbalance having started in the fifth decade. In four patients, cough preceded gait imbalance between 15 and 29 years of age; the cough was spasmodic and triggered by variable factors. In addition, vestibular function tests showed bilateral impairment of the vestibulo-ocular reflex.
The presence of chronic spasmodic cough, in this study, for over 10 years even before balance and postural disturbances showed up, suggest that machine language, as repeatedly exposed in the specific chapters of Masticationpedia, is a reality not to be overlooked because the ambiguous and vague verbal language covers the information of the encrypted code. As we will demonstrate in the course of the discussion, the analog of the spasmodic cough symptom of the patients reported by Jon Infante's article could be the repeated reporting to the dental colleagues of the chewing difficulty by our patient 'Balancer'. (Figure 2) This parameter has not been considered as an 'encrypted code' but only an element of verbal language logic and therefore vague and ambiguous. The continuous remaking of the prosthetic rehabilitation dampened even more the information of the machine language until the temporal and spatial addition of the organic damage was transformed[1] into a macroscopic symptom of vertigo and loss of balance in walking

Jon Infante's article[1] concludes with a striking statement, i.e. that spasmodic cough can be an integral part of the clinical picture in CANVAS, anticipating the appearance of postural imbalance by several decades and that sparing of muscle spindle afferents (Ia fibers) is probably the pathophysiological basis of normoreflexia.
(........is the neurological damage functional or organic?)
Decryption process
The diagnostic procedure followed routinely according to the Masticationpedia model has allowed us to eliminate, through the coherence demarcator, the dental context to follow the neurological one and to deepen through the 'Cognitive Neural Network' (CNN) the possible correlations between symptoms and neurophysiological abnormalities in patients with postural and walking disorders due to functional pathologies (labyrinthitis, neuropathies, etc.) from organic ones (tumors, demyelinations, etc.). Now we must try to decrypt the encrypted message of the machine language of the Trigeminal Nervous System.
Encrypted code

As anticipated, first of all we were able to highlight a serious absence of the jaw jerk reported as Abnormality, positive report (Figure 1) but as already mentioned in the chapter

' Conclusions on the status quo in the logic of medical language regarding the masticatory system' also in the patient treated with orthognathic surgery we were able to detect an absence of the jaw jerk (figure 2) restored immediately after evoked neurognathological rehabilitation. In our case 'Balancer' we have an additional objective disorder that of masticatory difficulty and together with the postural disorder there were nystagmus and vertigo.
A further assertion in favor of organic damage was also the presence of a latency delay on the right side of the electrical silent period, Abnormality, positivity of the report, which suggests a slowing of the nerve conduction speed. In this instance we cannot say whether the delay refers to damage to the sensory or motor fibers until we approach the study of the nerve conduction of the motor trigeminal roots.

Motor evoked potentials of the trigeminal root


In our masticatory neurophysiology laboratory we have developed a technique of electrical transcranial electrostimulation of the two trigeminal roots simultaneously and synchronized with the electrical stimulus. In the various chapters already published some technical information on the method is reported but we intend to expose them exhaustively in the section 'Extraordinary science'. In this context we can only consider and confirm a significant amplitude asymmetry of the motor evoked responses as shown in figure 3. The markers 1A and 2A indicate the latency which, unlike the silent period, is symmetrical and this data confirms the structural damage of the sensory fibers including those proprioceptive from masticatory muscles. At this point we can not only confirm and justify the neurological choice of the diagnostic context but also conclude with a pre-diagnosis of cerebellar neurological damage with involvement of the trigeminal mesencephalic axis.
The Magnetic Resonance of the brain, unfortunately, solves our doubts with a report of solid expansive lesion with mass effect in the right hemisphere, it is not clear whether it has a supra or sub tentorial origin, it certainly determines compressive phenomena on the midbrain - trunk and on the fourth ventricle with dilatation of the cisternae and ventricles upstream. That it is a meningioma is very likely because he has no perilesional edema.
Final considerations
We summarize the clinical diagnostic path following the Masticationpedia model so that the latter can be considered a fluid and dynamic process to reach a diagnostic target in the fastest and most detailed way.
- Context analysis through dental and neurological laboratory tests
- Choice of neurological statement filtered by the Coherence Demarcator
- Evaluation of the clinical case in the Cognitive Neural Network (CNN)
- Closing the CNN loop with Jon Infante's article[1] and the consideration of the organic/functional damage of our patient's trigeminal sensory-motor structures through the observation of the amplitude asymmetry of the 'bRoot-MEPs'. The logical sequence of the tests carried out with the numbering restored has been ordered in the image gallery.
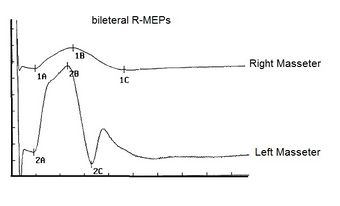
Figure 1a: The first test that must always be performed in complex clinical cases is, in fact, the bRoot-MEPs
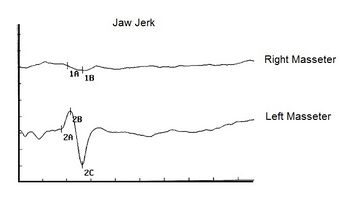
Figure 1b: The second test is the jaw jerk which returns a sort of analysis of the integrity of the midbrain system. In our case 'Balancer' an abnormal asymmetry is evident to the detriment of the right masseter
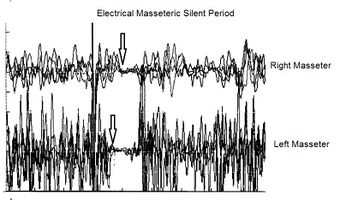
Figure 1c: After verifying the level of integrity of the midbrain area through tests involving monosynaptic reflexes such as jaw jerk, the level of complexity is raised by evoking the electrical silent period which is a polysynaptic reflex. The latency delay on the right masseter is evident
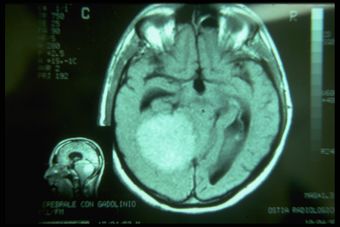
Figure 1d: Obviously after these results, the patient cannot be considered affected by postural disorder but by organic neurological pathology and the Nuclear Magnetic Resonance of the brain shows it in all its diagnostic potential.



Conclusion
We now have evidence of both direct and indirect functional organic correlation between the trigeminal system and the vestibular system, just think of the study of mVEMP (Vestibular Evoked Myogenic Potentials) now recognized as a solid and reliable test for assessing the functional integrity of the reflex pathway vestibulo-masseteric[4] in clinical manifestations with involvement of the trigeminal and vestibular system as in schwannomas[5][6] or in the presence of acoustic neuromas[7] as much as the relative correlation between dental occlusion and the vestibular system but this does not allow, given the seriousness of the diagnostic error that it would result, to consider this last clinical condition a clinically validated scientific datum. In the Appendix an example of what might happen.
This last assertion, perhaps risky because it is controversial, collides with the evidence of a striking fact highlighted several times during the drafting of the chapters of Masticationpedia, that of machine language and verbal language. A vague and ambiguous verbal language can generate scientific convictions depending on how it is proposed but in substance it covers and hides a much more decisive and formal machine language. For example, the verbal language deduced that the postural disturbances of the 'Balancer' patient were caused by an incongruous prosthetic rehabilitation while the machine language signaled an organic sensorineural deficit (absence of the jaw jerk, latency delays of the silent period, large reduction in the amplitude of the bRoot-MEPs.
The lack of information on the velocity and the mandibular position at the midbrain level, in fact, determines an incapacity of stereognostic awareness in which the patient does not recognize the spatial and temporal position of the mandible. The decrease in the recruitment of the motor units of the masticatory muscles and not only of the tested masseter with an obvious decrease in the masticatory force is the result of this organic and functional damage. All this indicates an impairment of the proprioceptive territory but we do not know if the sensory structures have also been involved. The electrical silent period, on the other hand, shows a severe delay in latency with a slowing of nerve conduction velocity. To conclude the neurophysiopathological diagnostic picture is the observation that the right trigeminal motor root has lost most of its motor fibers.
However, it should be noted that in such a serious clinical condition we see a decrease in the amplitude of the bRoot-MEPs but not a latency asymmetry. This finding indicates that there was direct damage to the trigeminal motor fibers from tumor compression (axonotmesis) but not demyelination (neuropraxia) which would have shown latency delay on the right masseter. It is advisable to briefly describe the definition of neurological damage bearing in mind that the equivalent of the spinal peripheral nerve for the trigeminal nervous system corresponds to the motor trigeminal root.
Neurotmesis is caused by a transection of a nerve and is the worst degree of peripheral nerve injury. In neurotmesis, the entire nerve, including the endoneurium, perineurium, and epineurium, is completely severed. Neurotmesis leads to disruption of the axon, myelin sheath, and connective tissues. The prognosis for spontaneous recovery is poor without surgery.[8] Sunderland's fifth-degree lesion fits the definition of neurotmesis in the Seddon classification and represents the highest degree of nerve injury, with a complete nerve defect.
Neurapraxia is a nerve injury commonly induced by focal demyelination and/or ischemia and is the mildest type of peripheral nerve injury. In neurapraxia, nerve impulse conduction is blocked in the injured area, sensory and motor connection is lost, but all morphologic structures of the nerve stump, including the endoneurium, perineurium, and epineurium, remain intact.
Axonotmesis is a relatively more serious type of peripheral nerve injury and is usually caused by crushing, stretching, or percussion. In axonotmesis, the epineurium is intact, while the perineurium and endoneurium may be disrupted. The axon is separated from the soma and the axon and myelin sheath are disrupted. Wallerian degeneration occurs in the axon stump distal to the injury site within 24 to 36 hours after peripheral nerve injury.
After neurotmesis, Schwann cells respond adaptively to axonal disruption, transitioning from a highly myelinated state to a dedifferentiated state. De-differentiated Schwann cells engulf axons and myelin debris and form a regenerative pathway for axon outgrowth. Additionally, activated Schwann cells secrete a group of cytokines, including tumor necrosis factor-alpha, interleukin-1 alpha, and leukemia inhibitory factor, to recruit macrophages and facilitate digestion of debris. Schwann cells also secrete a group of neurotrophic factors, including nerve growth factor, brain-derived neurotrophic factor, and glial cell line-derived neurotrophic factor, to encourage neuron survival and axon elongation.[9][10][11]
Needle electromyography (EMG) is the most sensitive electrodiagnostic study for motor axon loss, and low-amplitude motor responses appear with severe injuries. Decrease in motor response amplitude begins around days 2-3 and is complete by day 6. This reflects the fact that neuromuscular junction degeneration precedes axon degeneration and motor responses are dependent on neuromuscular junction transmission.[12]
Appendix
Patient treated by a dental colleague for a prosthetic rehabilitation following postural methods which indicated the best Centric occlusion through dynamometric platforms. The patient came to our observation presenting a clinical state of fasciculation of the masseter muscles as well as, obviously, an occlusal and masticatory discomfort. The centric position finalized by the colleague was, therefore, correlated with the best postural dynamometry response but unfortunately this did not result.
Observing figures 5,6 and 7 we can understand how axioms are built that do not respond to a validated scientific criterion, much less to a biological reality. Thinking that a remote phenomenon such as postural stability dictated by a dynamometric platform can validate the choice of a position occlusal achieved manually by the operator breaks down on the observation that by observing the state of the trigeminal system by measuring it through a demand (bRoot-MEPs) the system responds with its own spatial position not dictated by posturological correlation nor by the manual maneuvers of the operator but by its own vectorial neuromotor result.

Figure 5: Rehabilitated patient following posturological indications from dynamometry data.

Figure 6: Centric occlusion defined through data indications of the dynamometric platform.

Figure 7: Centric position resulting from bRoot-MEPs. Note the retrusion of at least 3mm and the leftward displacement of the mandible.



{kind=link}
{kind=link}
(….should only be considered as an experimental exploratory field to deduce more knowledge on neuronal connectivity.)
- ↑ 1.0 1.1 1.2 1.3 1.4 Jon Infante, Antonio García, Karla M Serrano-Cárdenas, Rocío González-Aguado, José Gazulla, Enrique M de Lucas, José Berciano. Cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS) with chronic cough and preserved muscle stretch reflexes: evidence for selective sparing of afferent Ia fibres.J Neurol . 2018 Jun;265(6):1454-1462. doi: 10.1007/s00415-018-8872-1.Epub 2018 Apr 25.
- ↑ The history of examination of reflexes. Boes CJ.J Neurol. 2014 Dec;261(12):2264-74. doi: 10.1007/s00415-014-7326-7. Epub 2014 Apr 3.PMID: 24695995
- ↑ Chen Y, Gong X, Ibrahim SIA, Liang H, Zhang J.. Convergent innervations of mesencephalic trigeminal and vestibular nuclei neurons onto oculomotor and pre-oculomotor neurons-Tract tracing and triple labeling in rats. PLoS One. 2022 Nov 28;17(11):e0278205. doi: 10.1371/journal.pone.0278205. eCollection 2022.PMID: 36441755
- ↑ Sangu Srinivasan Vignesh, Niraj Kumar Singh, Krishna Rajalakshmi. Tone Burst Masseter Vestibular Evoked Myogenic Potentials: Normative Values and Test-Retest Reliability. J Am Acad Audiol. 2021 May;32(5):308-314. doi: 10.1055/s-0041-1728718.Epub 2021 Jun 1.
- ↑ Ashutosh Kumar, Sanjay Behari, Jayesh Sardhara, Prabhaker Mishra, Vivek Singh, Vandan Raiyani, Kamlesh Singh Bhaisora, Arun Kumar Srivastava . Quantitative assessment of brainstem distortion in vestibular schwannoma and its implication in occurrence of hydrocephalus.Br J Neurosurg . 2022 Dec;36(6):686-692. doi: 10.1080/02688697.2022.2047155.Epub 2022 Mar 7.
- ↑ Daniel Moualed, Jonathan Wong, Owen Thomas, Calvin Heal, Rukhtam Saqib, Cameron Choi, Simon Lloyd, Scott Rutherford, Emma Stapleton, Charlotte Hammerbeck-Ward, Omar Pathmanaban, Roger Laitt, Miriam Smith, Andrew Wallace, Mark Kellett, Gareth Evans, Andrew King, Simon Freeman. Prevalence and natural history of schwannomas in neurofibromatosis type 2 (NF2): the influence of pathogenic variants. Eur J Hum Genet. 2022 Apr;30(4):458-464. doi: 10.1038/s41431-021-01029-y.Epub 2022 Jan 24.
- ↑ Claudia Cassandro, Roberto Albera, Luca Debiasi, Andrea Albera, Ettore Cassandro, Alfonso Scarpa, Massimo Ralli. What factors influence treatment decision making in acoustic neuroma? Our experience on 103 cases. Int Tinnitus J. 2020 Nov 18;24(1):21-25.doi: 10.5935/0946-5448.20200004.
- ↑ Kaya Y, Sarikcioglu L. Sir Herbert Seddon (1903-1977) and his classification scheme for peripheral nerve injury. Childs Nerv Syst. 2015 Feb;31(2):177-80.
- ↑ Jessen KR, Mirsky R, Lloyd AC. Schwann Cells: Development and Role in Nerve Repair. Cold Spring Harb Perspect Biol. 2015 May 08;7(7):a020487.
- ↑ Madduri S, Gander B. Schwann cell delivery of neurotrophic factors for peripheral nerve regeneration. J Peripher Nerv Syst. 2010 Jun;15(2):93-103.
- ↑ Yi S, Zhang Y, Gu X, Huang L, Zhang K, Qian T, Gu X. Application of stem cells in peripheral nerve regeneration. Burns Trauma. 2020;8:tkaa002
- ↑ Ferrante MA. The Assessment and Management of Peripheral Nerve Trauma. Curr Treat Options Neurol. 2018 Jun 01;20(7):25.